

Idea #160
Managing Risks: Culture Matters More Than Rules
To gain access to all Ideas for Leaders content please Log In Here or if you are not already registered then Register Here.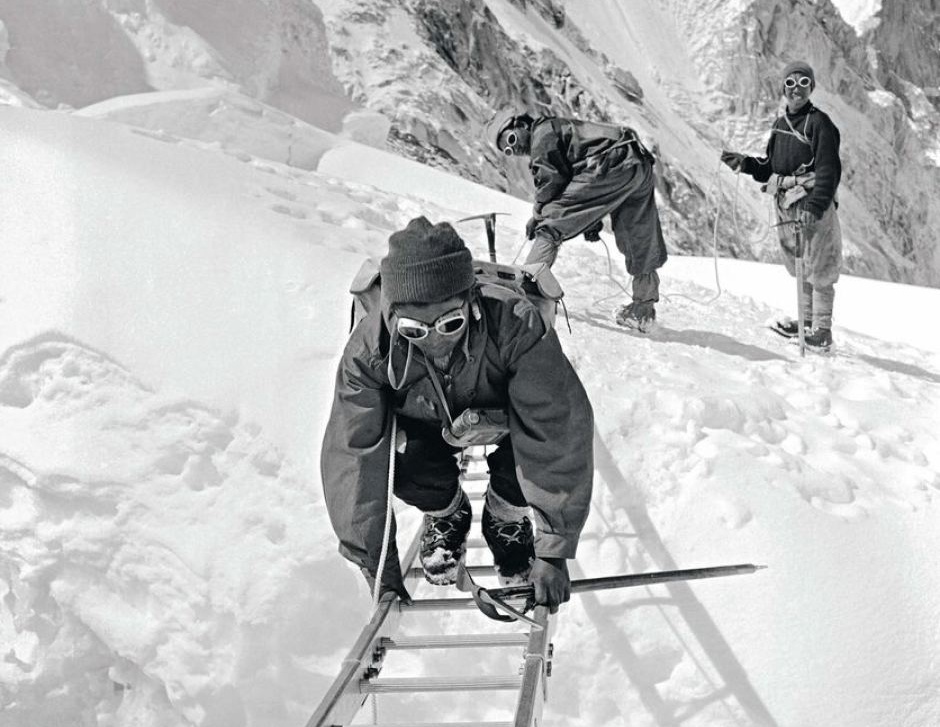
Main Image





